

INTRODUCTION
Bladder cancer (BC) is the tenth most prevalent cancer globally, with an annual incidence of approximately 573,000 cases, and 213,000 deaths [1]. The most common subtype is urothelial BC. Approximately 75% of patients initially present with non-muscle-invasive bladder cancer (NMIBC) confined to the bladder mucosa and submucosa [2,3]. Treatment of NMIBC primarily consists of localized treatment and surveillance. The high prevalence of this stage is due to its nonaggressive characteristics. In cases of NMIBC with a high risk of cancer recurrence and progression, adjuvant intravesical instillation of bacillus Calmette-Guérin (BCG) immunotherapy is considered [2,3].
Intravesical BCG instillation after transurethral resection of bladder tumor (TURBT) has been demonstrated to decrease recurrence significantly [4]. However, recurrence is identified within 5 years of starting BCG treatment in approximately half of high-risk cases, and the prognosis for patients with BCG treatment failure is poor [5-7]. Several guidelines recommend radical cystectomy (RC) for patients who develop carcinoma in situ (CIS) and/or high-grade tumor recurrence despite sufficient BCG therapy due to the significant risk of disease progression [2,3].
However, as RC can degrade the quality of life [8], many patients opt for bladder preservation. Furthermore, many patients suffer from concurrent illnesses such as cardiovascular or pulmonary diseases due to tobacco exposure, which makes them unsuitable candidates for RC. Hence, there is a clinical need for alternative bladder-preserving treatments for patients with NMIBC who do not respond to BCG.
Pembrolizumab, a U.S. Food and Drug Administration (FDA)-approved immune checkpoint inhibitor (ICI), is an IgG4 anti-programmed cell death protein 1 (PD-1) humanized antibody. It functions by attaching to PD-1, thereby blocking the binding between PD-1 and its ligands, programmed death-ligand 1 (PD-L1) and programmed death-ligand 2. FDA approval was granted based on a randomized, phase 3 trial known as KEYNOTE-045, which was an open-label study that assigned 542 randomly selected patients who had recurrence or progression following platinum therapy [9]. Pembrolizumab also gained approval as a first-line therapy for cisplatin-ineligible patients with metastatic urothelial carcinoma based on early data from the phase 2 KEYNOTE-052 study [10,11].
The KEYNOTE-057 study demonstrated that pembrolizumab monotherapy was well tolerated and showed promising results in patients with BCG-unresponsive NMIBC who were unsuitable for or refused RC [12]. Consequently, it should be considered as a clinically active nonsurgical treatment alternative for this challenging patient population. In this study, we investigated the efficacy of pembrolizumab, a PD-1 inhibitor, in patients with NMIBC that was unresponsive to intravesical BCG administration in a real-world setting.
MATERIALS AND METHODS
This study was approved by the Institutional Review Board of the Samsung Medical Center (IRB No. 2023-07-146-001), which waived the requirement for informed consent because of the retrospective nature of this study. All the study protocols were performed in accordance with the principles of the Declaration of Helsinki.
We retrospectively reviewed the records of patients who experienced recurrence after BCG treatment and subsequently received pembrolizumab treatment between December 2016 and February 2023. Patients who experienced recurrence after intravesical BCG instillation were included in this study. They were pathologically diagnosed with urothelial carcinoma by TURBT before intravesical BCG instillation, and NMIBC was confirmed by TURBT before pembrolizumab administration. Among the included patients, 1 patient was diagnosed with muscle-invasive BC at the first TURBT; however, the patient wanted bladder preservation. Intravesical BCG instillation was performed as part of the treatment, and then NMIBC was confirmed by TURBT before pembrolizumab administration.
When intermediate-to-high NMIBC was confirmed after TURBT, intravesical BCG induction was initiated and performed 6 times weekly. After intravesical BCG induction, the response was evaluated through a cystoscopic examination with or without biopsy after 3 months. Depending on the response, a second intravesical BCG induction or intravesical BCG maintenance was performed 3 times weekly, and after 3 months, post-BCG cystoscopic examination with/without biopsy was used to evaluate the response. In the absence of recurrence, intravesical BCG maintenance was continued every 6 months.
BCG-unresponsive NMIBC was defined as persistent CIS, high-grade Ta tumors, or high-grade T1 tumors at 6 months after receiving adequate BCG therapy. Adequate BCG therapy referred to the administration of at least 5 of 6 induction doses and 2 of three maintenance treatments of BCG, or at least 2 of 6 instillations of a second induction course when maintenance BCG was not provided.
The definition of BCG-unresponsive NMIBC also included patients who experienced recurrences of high-grade Ta or T1 NMIBC within 6 months, or CIS within 12 months following a disease-free state after BCG treatment; patients who continued to exhibit persistent high-grade Ta or CIS, or showed progression to T1 disease after BCG therapy, were also considered to have BCG-unresponsive NMIBC.
Patients with BCG-unresponsive NMIBC received intravenous pembrolizumab 200 mg every 3 weeks. We evaluated the patient’s response to pembrolizumab therapy via urine cytology, cystoscopic examination (with/without biopsy), and/or CT imaging after 4 administrations. Patients were followed up every 3 months for the first 2 years and every 6 months thereafter. The primary endpoint was the complete response (CR) rate 3 months after the first dose of pembrolizumab. Secondary outcomes included duration of response, progression-free survival, complications, and recurrence after pembrolizumab treatment.
Descriptive statistics included frequencies and proportions of categorical variables. Continuous variables are presented as median (range). Kaplan-Meier survival analysis was used to illustrate CR and demonstrate the individual treatment course. All statistical analyses were performed using IBM SPSS Statistics ver. 27.0 (IBM Co., Armonk, NY, USA).
RESULTS
1. Baseline Characteristic
In total, 24 patients who experienced recurrence after BCG treatment and subsequently underwent pembrolizumab treatment were analyzed. As shown in Table 1, the median age was 70.5 years (range, 47-85 years), and 5 patients had a history of surgery for upper urinary tract carcinoma (3 and 2 patients had underwent radical nephroureterectomy and distal ureterectomy, respectively). Eight patients (33.3%) had CIS on the initial TURBT, and 15 patients (62.5%) had CIS on TURBT just before the administration of pembrolizumab. The median number of pembrolizumab administration was 5 times (range, 3-39 times) and the duration was 3 months (1-64 months). The total follow-up period was 16 months (2-68 months).
2. Response to Pembrolizumab
The primary outcome, CR at the first assessment (usually 3 months after pembrolizumab administration), was observed in 54.2% (13 patients) in this study. CR was maintained for 15 months (range, 5-47 months) in these patients. Eleven patients (45.8%) showed CR at the second assessment (usually 6 months after pembrolizumab administration). Five patients (20.8%) maintained a recurrence-free status 1 year after pembrolizumab administration (Table 2).
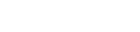
The median duration of CR at onset was 22 months (95% confidence interval, 9.1-34.9), and 5 of 13 patients (38.5%) had CR for 12 months or longer (Fig. 1). The detailed responses and clinical courses of the individual patients are shown in Fig 2.
Eight patients (33.3%) experienced adverse events following pembrolizumab administration. Fatigue was the most common symptom, followed by pruritus, and features of hyperthyroidism (Table 3).
3. Treatment for Patients With Recurrence After Pembrolizumab
No CR was observed in 11 patients during the first assessment. Eight patients (72.7%) either underwent RC or planned RC (Fig. 2). Three patients either planned or underwent other intravesical therapies, including gemcitabine and mitomycin.
In total, 7 patients (29.2%) underwent RC because of recurrence after pembrolizumab administration. There was no aggravation of pathological results after TURBT when comparing the pathology before RC with that before pembrolizumab administration. When comparing the pathology of RC with that before pembrolizumab administration, aggravation of pathology was observed in 3 patients (Table 4).
DISCUSSION
Although platinum-based combination chemotherapy continues to be the primary treatment for advanced BC, the surge in the understanding of the biological intricacies of BC has spurred a growing interest in ICIs and molecularly targeted treatments [13]. BC is characterized by frequent mutations [14], and its high tumor mutational burden makes it susceptible to ICIs targeting PD-1 and its ligand, PD-L1 [15,16]. Consequently, ICIs that inhibit PD-1 or PD-L1 have gained FDA approval for the first- and second-line treatment of metastatic BC.
Additionally, a role for the PD-1-PD-L1 pathway in fostering resistance to BCG in NMIBC has been proposed. Tumors that have recurred or progressed following BCG treatment have been found to exhibit a noticeable increase in PD-L1 expression compared to tumors that have never been treated with BCG. Furthermore, increased PD-L1 expression has been associated with recurrence and progression [17].
Despite RC being recommended as a treatment option for BCG-unresponsive NMIBC by several guidelines [2,3], the demand for alternative treatments has surged because of the high complication rate associated with RC and patients’ preference for preserving the bladder. Based on the findings of the PD-L1 study, pembrolizumab is expected to be a viable treatment option for BCG-unresponsive NMIBC.
This study aimed to investigate the efficacy of pembrolizumab in patients with NMIBC who did not respond to intravesical BCG instillation through our initial experience. The tolerability and antitumor activity of pembrolizumab in patients with BCG-unresponsive NMIBC were reported in the KEYNOTE-057 study [12]. However, there have been no studies on pembrolizumab in patients with NMIBC in a clinical setting. In real clinical situations, a patient’s disease state is not constant, and there are various factors to be considered. Our study demonstrated the efficacy of pembrolizumab in patients with BCG-unresponsive NMIBC.
In our study, the primary outcome, CR at the first assessment (usually at 3 months after pembrolizumab administration), was observed in 54.2% of patients; among them, 38.5% maintained a recurrence-free status at 1 year after pembrolizumab administration. The KEYNOTE-057 study showed a 41% CR rate at 3 months after the administration of pembrolizumab for patients with BCG-unresponsive CIS of the bladder with or without papillary tumors, and 46% of responders remained in CR for 12 months or longer [12]. In terms of complications, 33.3% of patients had treatment-related adverse events in our study, and 66% of patients had treatment-related adverse events in KEYNOTE-057. Our study showed better results than the KEYNOTE-057 study.
Additionally, we analyzed the pathological results of patients who underwent RC after the failure of pembrolizumab treatment. Seven patients underwent RC; among them, 3 patients showed upgrading of T stage to T2, and 1 patient showed downgrading of T stage to TX. Although the patients experienced aggravation of the disease stage, they were able to receive appropriate treatment by undergoing RC. Therefore, the period before surgical treatment can be extended by administering pembrolizumab. Although pembrolizumab treatment results in failure of disease control, it can be properly managed by RC, and we can confirm that pembrolizumab could affect pathological complete remission. Therefore, clinicians should consider pembrolizumab administration to patients with BCG-unresponsive NMIBC.
Previous studies suggest a variance in the 1- to 2-year recurrence-free survival rates, ranging from 18% to 43%, following diverse salvage therapies in patients experiencing BCG treatment failure [18-23]. Consequently, the International Bladder Cancer Group posits a benchmark for clinical significance, advocating for an initial CR rate of 50% at the 6-month interval, coupled with sustained response rates of 30% at 12 months and 25% at 18 months in patients with BCG-unresponsive CIS. In instances of BCG-unresponsive papillary disease, recurrence-free benchmarks of 30% at 12 months and 25% at 18 months are deemed clinically significant [5]. Our study, albeit lacking a control cohort of NMIBC patients not treated with pembrolizumab, demonstrates that pembrolizumab surpasses the efficacy of extant salvage therapies, aligning with the recommendations of the International Bladder Cancer Group.
Some studies have attempted to demonstrate the efficacy of novel treatment options in patients with BCG-unresponsive NMIBC. One concerns hyperthermic intravesical chemotherapy for BCG-unresponsive NMIBC. The study reported that the 3-month, 6-month, 9-month, and 1-year cumulative incidence rates of disease recurrence/progression were 25%, 35%, 44%, and 53%, respectively [24]. Another option is intravesical gemcitabine treatment. There have been some reports on intravesical gemcitabine use in patients with NMIBC with recurrence after intravesical BCG instillation. Hurle et al. [25] reported a disease-free survival rate of 68.8% after induction (once a week for 6 consecutive weeks) and 44.4% disease-free survival after 12 months of treatment. Skinner et al. [19] reported 47% and 28% CR rates at 3 and 12 months, respectively. Another study reported on intravesical nadofaragene firadenovec gene therapy for BCG-unresponsive NMIBC. Boorjian et al. [26] reported 53.4% and 45.5% CR rates at 3 and 12 months, respectively, after initial administration. Direct comparison between these treatments is difficult because each study has a different group of patients and research methods; however, based on the results of our study, it can be suggested that pembrolizumab can also be considered as a treatment option in patients with BCG-unresponsive NMIBC.
Despite the strengths of this study, it has several limitations. First, the retrospective design may have resulted in a significant selection bias. Second, it is limited to establishing the effect of pembrolizumab, and additional analysis of factors such as treatment success was not possible due to the relatively small cohort. Third, the patients were not uniform in terms of tumor characteristics or previous therapy. Additionally, the absence of PD-L1 testing in this study represents a missed opportunity for more detailed understanding of pembrolizumab’s clinical implications. Further, well-designed studies are required to determine the clinical significance and efficacy of pembrolizumab therapy in patients with BCG-unresponsive NMIBC.
CONCLUSIONS
Our early experience with pembrolizumab treatment for BCG-unresponsive NMIBC showed better results than those of the KEYNOTE-057 trial. Pembrolizumab treatment can be considered in patients with BCG-unresponsive NMIBC who decline or are not eligible for RC. However, long-term data and more cases are needed to establish pembrolizumab treatment for patients with BCG-unresponsive NMIBC in real-world settings.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print



