

INTRODUCTION
Urologists and radiologists should be familiar with the Prostate Imaging and Reporting and Data System (PI-RADS) for effective communication. At present, PI-RADS version 2.1 (PI-RADSv2.1) is available for clinical use and aids in risk stratification for prostate cancer in men with elevated prostate-specific antigen (PSA) levels [1-3]. This system recommends suitable sequences, protocols, and MRI interpretations, and urges urologic cancer centers to adhere to these for standardization. Consequently, it assists in standardizing image quality and interpretations between radiologists and urologists. However, interpreting MRI scans using the PI-RADSv2.1 decision rules often presents significant diagnostic challenges. There are few reports addressing the limitations of applying PI-RADSv2.1 in clinical practice. The aim of this review is to outline the limitations that should be understood when using the current PI-RADSv2.1 in a clinical setting.
TUMOR SIZE
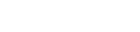
Like PI-RADSv2.0 [4-6], PI-RADSv2.1 [1-3] also suggests 1.5 cm as a cutoff value to discriminate between categories 4 and 5 (Tables 1, 2). This value, however, is not derived from evidence-based research, but rather from expert consensus [7, 8]. The rationale behind establishing 1.5 cm as the size cutoff for category differentiation is not clear to radiologists or urologists. Some researchers have suggested that a cutoff of 1.0 cm might be more effective in differentiating between categories 4 and 5 [7, 8]. Park and Park [8] found that larger PI-RADS 4 tumors (≥1 cm) had a significantly higher cancer detection rate than smaller ones (<1.0 cm). However, they also showed that there was no significant difference in the cancer detection rate between PI-RADS 4 tumors (≥1.0 cm and <1.5 cm) and PI-RADS 5 tumors (≥1.5 cm) [8]. Therefore, it may be beneficial to lower the size cutoff to 1.0 cm for differentiating between PI-RADS 4 and 5 (Fig. 1).
Moreover, there is still no clear consensus on how and where to measure a lesion [1-3]. Diffusion-weighted imaging (DWI) can illustrate the degree of diffusion restriction, but it fails to provide detailed anatomical information in high b-value images. In contrast, T2-weighted imaging (T2WI) can reveal the anatomical details of a lesion, but it lacks the ability to provide functional information. Given these characteristics, T2WI is generally more accurate than DWI for measuring lesion size. According to PI-RADSv2.1, DWI is the preferred method for assessing peripheral lesions, while T2WI is recommended for evaluating transition lesions [1-3]. Therefore, the size of a peripheral lesion should ideally be measured using DWI, and the size of a transition lesion should be measured using T2WI. However, size measurements can often be under- or overestimated on DWI due to frequent image distortions caused by artifacts (Fig. 1). Furthermore, MR images can be obtained in 3 dimensions, regardless of the MRI sequences used. Yet, PI-RADSv2.1 does not specify the imaging plane on which the lesion size should be measured. The choice of magnetic resonance (MR) sequences and imaging planes varies from one institution to another. For instance, a lesion that measures less than 1.5 cm on an axial image could measure 1.5 cm or more on a coronal or sagittal image. Not every imaging plane can be obtained on T2WI or DWI.
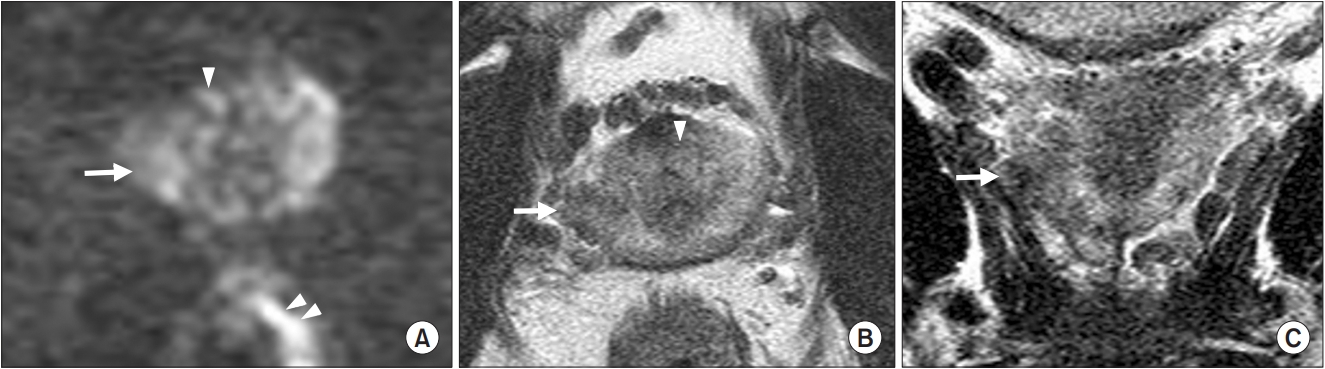
PI-RADSv2.1 has another pitfall in assessing transition lesions. Both DWI findings and T2WI contribute to its classification. Typically, radiologists or urologists understand that a PI-RADS 4 lesion is smaller than 1.5 cm. However, according to PI-RADSv2.1 decision rules, a PI-RADS 4 lesion can measure 1.5 cm or larger [1-3]. If a transition lesion measures 1.5 cm or more and is significantly hyperintense on DWI, it is classified as PI-RADS 4 (Fig. 2) [9]. This decision rule often confuses radiologists and urologists, making it difficult for them to accurately classify or distinguish between PI-RADS 4 and 5 [9].
SIGNAL INTENSITY
The definitions of signal intensity for a lesion on T2W or DW images in PI-RADSv2.1 remain somewhat vague (Tables 1, and 2). The system merely describes signal intensity as weak, intermediate, or strong for each category, which can be subjective and lead to significant discrepancies between observers. PI-RADSv2.1 decision rules lack absolute or relative quantitative or qualitative values [1-3]. Therefore, there is a need to redefine the signal intensity of a lesion in relation to the highest or lowest signal intensity of other prostate tissue. It’s not feasible to propose an absolute value for a lesion due to varying references across commercially available MRI scanners. However, we can compare a lesion to other prostate tissues, with benign prostate hyperplasia (BPH) nodules serving as the best reference (Fig. 1). These nodules exhibit the lowest or highest signal intensity on T2W or DW images. If the signal intensity of a peripheral lesion matches that of a BPH nodule with the highest signal intensity, we can classify it as PI-RADS 4 or 5 on DW images. If the signal intensity of a peripheral lesion falls between the lowest and highest signal intensities of BPH nodules, we can describe it as moderately hypointense on T2W images.
TUMOR MORPHOLOGY
The morphology of a tumor plays a crucial role in distinguishing between significant and insignificant cancers. The PI-RADSv2.1 system outlines the shapes of PI-RADS 2 peripheral and PI-RADS 1-4 transition lesions, as detailed in Tables 1 and 2 [1-3]. A PI-RADS 2 peripheral lesion is typically linear or wedge-shaped, while the other categories do not provide specific morphological information. PI-RADS 1-4 transition lesions exhibit varying morphologies, depending on the degree of encapsulation (complete, partial, or obscured), the texture of the tumor (homogeneous or heterogeneous), and whether they are lenticular or nonlenticular. However, these decision-making rules can be perplexing for radiologists when it comes to classifying a lesion. For instance, a transition nodule that is mostly encapsulated is classified as PI-RADS 2. Yet, this rule does not take into account signal intensity, tumor texture, or whether the lesion is lenticular or nonlenticular. Consequently, if a mostly encapsulated transition nodule is moderately hypointense, lenticular, or homogeneous, it is unclear whether it should be classified as PI-RADS 2 or 4. The PI-RADSv2.1 system does not provide explicit descriptions of the detailed morphologies for each category. As the margin of a tumor becomes well-defined and smooth, it is more likely to be an insignificant cancer. Conversely, if the tumor margin is poorly defined and irregular, it is more likely to be a significant cancer, as illustrated in Fig. 1 [10].
The current Breast Imaging and Reporting and Data System (BI-RADS) provides a detailed description of tumor morphology, including aspects such as margin, contour, and size ratio [11-13]. However, PI-RADSv2.1 does not offer as comprehensive guidelines on morphology as BI-RADS does. It relies solely on MR images, and the diagnostic results can vary based on the resolution of these images and their interpretation. High-quality resolution and accurate interpretation of MR images lead to improved outcomes in the detection, assessment, and staging of prostate cancer. Therefore, future versions of PI-RADS should include more detailed descriptions of tumor morphology, such as size, shape, contour, and margin. To ensure the quality and appropriate interpretation of MRI, radiologists and urologists should participate in annual refresher training courses.
TUMOR LOCATION
PI-RADSv2.1 advocates for the use of a segmentation model, which comprises 41 sectors/regions: 38 designated for the prostate, 2 for the seminal vesicles, and 1 for the external urethra [1-3]. The aim is to facilitate effective communication between radiologists, urologists, and pathologists using a sector map. In theory, this appears beneficial for lesion localization. However, there is considerable disagreement, even among radiologists, regarding lesion localization using these sector map rules. Furthermore, each sector is demarcated by hypothetical lines, meaning that the tumor location can shift depending on the radiologist, urologist, or pathologist who is localizing it.
We propose that the classification of sectors can be simplified into right/left and anterior/posterior, based on the base, midgland, and apex [14]. This results in a total of 12 (2×2×3) sectors for the prostate. If a lesion is relocalized using 12 sectors after being localized with 38 sections, the sector map becomes easier to interpret due to the reduced number of sectors. This kind of sector map could provide a more straightforward method for radiologists, urologists, and pathologists to communicate with each other than the current method employed by PI-RADSv2.1.
MAGNETIC RESONANCE IMAGE QUALITY
At present, we have access to MR images from a variety of scanners, including 1.5 T/3.0 T and endorectal/surface coils. PI-RADSv2.1 accepts images from all these sources, provided they are scanned according to the specified protocols [15]. However, it raises the question of whether the image quality of 1.5 T MRI using a surface coil is equivalent to that of 3.0 T MRI using an endorectal coil. It is clear that the signal-to-noise ratio of the former is significantly lower than that of the latter. As a result, a lesion categorized as PI-RADS 2 or 3 on 1.5 T MRI is often upgraded to PI-RADS 4 or 5 on 3.0 T MRI. Furthermore, the superior image quality of DWI or T2WI can aid in the detection or characterization of a lesion when scanned using a 3.0 T MRI device. This allows us to evaluate a lesion with more detailed information regarding tumor detection, signal intensity, and morphology. The precision of the MRI diagnosis increases when a patient with a high PSA level is examined using a higher-strength MRI scanner. It is not uncommon for a prostate biopsy to be performed because a lesion is upgraded after assessment with 3.0 T MRI. However, PI-RADSv2.1 does not mandate the use of 3.0 T MRI for prostate assessment over 1.5 T MRI.
MAGNETIC RESONANCE IMAGING INTERPRETATION
It is widely recognized that there is significant variation among radiologists in their interpretation of MRI scans [16- 19]. However, PI-RADSv2.1 does not provide guidelines on how radiologists should be trained to use it. It remains unclear how frequently they should attend refresher courses or conferences, or at what intervals these should be undertaken. The number of MRI cases interpreted annually should be also unknown. It is not unusual for the PI-RADS category to be revised in a tertiary hospital after MR images from outside sources are reviewed by radiologists specializing in genitourinary imaging. This highlights a serious issue—namely, PI-RADSv2.1 does not set a minimum standard for radiologists who wish to interpret MR images.
CONCLUSION
The interpretation of MR images with PI-RADSv2.1 can present various pitfalls, as described above. Therefore, it becomes necessary to define lesions more clearly. This can be achieved by considering factors such as lesion size, signal intensity, morphology, location, and MR image quality. Regular education is also essential in this regard.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print



