

INTRODUCTION
Renal cell carcinoma (RCC) comprises approximately 3.8% of all new cancers, with a median age at diagnosis of 64 years [1]. Globally, it is the most frequently diagnosed renal malignancy [2]; approximately 85% of kidney tumors are RCC, and approximately 70% of these have a clear cell histology [3]. Other less common cell types include papillary, chromophobe, translocation, and Bellini duct (collecting duct) tumors [4]. Renal cancer is a malignant tumor caused by the cancerization of epithelial cells in different parts of the urinary tubules in the renal parenchyma. Its etiology is related to obesity, smoking, high blood pressure, long-term use of hormones, antipyretic and analgesic drugs, and other factors [5].
Partial nephrectomy (PN) is the preferred surgical approach for clinical T1 (cT1; ≤7 cm) renal masses, when technically feasible [6]. With great improvements in surgical technique, PN has become the preferred approach in the management of cT3 renal tumors [7]. PN not only yields similar efficacy with radical nephrectomy (RN) but also preserves nephrons to provide patients with a satisfactory postoperative quality of life [8]. However, when tumors are clinical stage T3—from preoperative imaging studies—the decision to perform a PN becomes difficult, although it is technically feasible. Furthermore, the efficacy of PN for deeply seated midline renal RCC, near the anatomically complex renal coronal plane and collecting systems remains controversial. If clinicians obtain more convincing evidence on the oncological safety and efficacy of PN in patients with pT3 RCC, it would be helpful in deciding a surgical strategy.
Previous studies suggested that PN and RN may provide oncological equipoise in pT3a RCC, with PN yielding better functional outcomes [9-11]. However, there is only one study that assessed patients renal vein thrombosis in cT3a RCC; no study had a long-term follow-up of over 10 years. In this study, we assessed for the statistical differences in the recurrence-free survival (RFS) and cancer-specific survival (CSS) for PN and RN, and accumulated evidence for PN in pT3a RCC without renal vein thrombosis over a long period.
MATERIAL AND METHODS
1. Patient Population
The study was approved by the Institutional Review Board (IRB) of Asan Medical Center (IRB No. 2022-1074) and the need for informed consent was waived. We retrospectively reviewed the charts of consecutive patients who underwent radical or PN for the treatment of clinical stage T1-3a renal tumors in our institute between January 2001 and December 2012. Patients with renal vein thrombosis, multiple, bilateral tumors, lymph node or distant metastases, or those who underwent systemic chemotherapy or pT1-2 RCC were excluded. Patients with renal vein thrombosis were excluded because they did not meet the criteria for PN. All types of surgical method (open, laparoscopic, and robotic surgeries) were included. Clinical stages were determined by the surgeon according to the patients’ documents and confirmed with a preoperative computed tomography (CT) or magnetic resonance imaging. All renal tumors were diagnosed pathologically as T3a RCC.
2. Data Collection
The demographic preoperative characteristics recorded included: age, sex, body mass index (BMI) and date of treatment. The operative details recorded included the surgical method, histologic type, pathological tumor size/stage, and surgical margin status. Patients were followed with contrast-enhanced CT of abdomen and pelvis at 3 months, after further 6 months and then annually. Blood tests including complete blood count, chemistry, electrolytes, and creatinine were done at baseline and at each follow-up visit.
3. Statistical Analyses
Patient demographics and tumor characteristics, including age, sex, tumor size, clinical stage, Fuhrman grade, histologic type and margin status, were evaluated and compared between the PN and RN using the Student t-test for continuous variables, and Pearson chi-square test for categorical variables analysis. The Kaplan-Meier survival curves and log rank test were used to investigate the RFS and CSS. The Cox proportional hazard regression models were used to identify the prognostic factors. A p-value of <0.05 was considered statistically significant, and all analyses were performed using IBM SPSS Statistics ver. 28.0 (IBM Co., Armonk, NY, USA).
RESULTS
1. Population Characteristics
A total of 149 patients who were diagnosed as pT3a RCC without existing renal vein thrombus were evaluated after PN and RN. Patient demographics and preoperative characteristics are reported in in Table 1. PN and RN were performed in 22 (14.8%) and 127 patients (85.2%), respectively. Relative to RN, patients who received PN showed smaller tumor size (3.1±1.7 cm vs. 7.0±2.9 cm, p<0.001) and lower clinical stage (p<0.001). Seventy-seven tumors (51.7%) upstaged to pT3a RCC from cT1-2 RCC. Histologically, 121 tumors (81.2%) were clear cell RCC, 5 tumors (3.4%) were papillary RCC, 14 tumors (9.4%) were chromophobe RCC, and 9 tumors (6.0%) were other RCC (sarcomatoid collecting duct carcinoma, granular RCC, cystic RCC, and Xp 11 translocation RCC). All patients were found to have negative margins (R0). 84 (56.4%) and 65 patients (43.6%) underwent open surgery and laparoscopic or robot surgery, respectively. Eighty tumors (66.2%) extended into the perinephric fat and 69 tumors (46.3%) extended into renal sinus. No differences were recorded in age, sex, BMI between the PN and RN groups (age: 61.1±9.8 years vs. 55.7±12.2 years, p=0.050; sex: 98 males vs. 51 females, p=0.218; BMI, 24.6±2.9 kg/m2 vs 24.7±3.3 kg/m2, p=0.765).
2. Recurrence and Survival Analysis
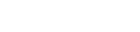
A total of 41 recurrences (27.5%) and 24 cancer related death (16.1%) were observed during a median follow-up of 136 months (interquartile range, 77-163 months). Figs. 1 and 2 show the Kaplan-Meier analysis for RFS and CSS in the 2 surgical groups. The mean time to cancer recurrence was 77.3±54.5 months (PN vs. RN: 85.4±64.0 months vs. 75.9±52.8 months, p=0.061). The mean time to cancer-specific death was 129.1±59.4 months (PN vs. RN: 153.2±52.5 months vs. 124.9±59.8 months, p=0.292). We observed no significant difference in RFS and CSS for PN and RN until the last follow-up visit. The tumor size (p<0.001) and BMI (p=0.036) were risk factors for RFS on univariate analysis (Table 2). On multivariate analysis, tumor size (hazard ratio [HR], 1.237; 95% confidence interval [CI], 1.132-1.350; p<0.001) was the only significant risk factor (Table 2). On multivariate analysis (Table 3), only tumor size remained associated with worse CSS (HR, 1.156; 95% CI, 1.027-1.302; p=0.017).
DISCUSSION
In the past 10 years, the application of PN to the management of patients with pT3a RCC has been explored, with increasing evidence to show that PN is safe and feasible for some T3a cases [10, 12]. However, the treatment of small renal masses has largely shifted to minimally invasive, nephron sparing surgery; treatment of larger masses and higher stage cancers are more controversial given that larger renal masses are more technically challenging and associated with unfavorable pathology [13]. Advancements in nephron sparing surgery have resulted in its application to managing pT3a RCC [6]. However, the application of PN to tumors with renal vein thrombus can be especially challenging; here, RN have historically been preferred [14]. Due to the surgical challenges in patients with renal vein thrombus, we except patient who estimated cT3a renal tumors with renal vein thrombus. In the present study, we report our experience with PN and RN for pT3a RCC without renal vein thrombus. Drawing from our extensive patient database, we focused on 22 pT3a PN and 127 RN cases. Of the 22 patients who had undergone PN, only 2 had disease progression and died of the disease. The other 20 patients (90.9 %) had no disease progression during a median follow-up period of 136 months. These rates did not differ significantly from those of the RN group. A univariate Kaplan-Meier plots did not show a difference in the rates of local recurrence, or disease-specific survival between the 2 surgery groups (Figs. 1, 2). We did not observe any difference in prognosis between the 2 surgical methods in patients with pT3a RCC without renal vein thrombus.
The indications for PN have broadened over the past decade [15-18]. The use of PN in patients with larger tumors has led to incidental diagnoses of perinephric fat invasion [19]. This finding might concern many urologists who encounter such pathology. Additionally, some may question whether a RN could result in better cancer control. Unfortunately, there are no clear data addressing such cancer control outcomes in patients with pT3a stage tumors who were treated with PN. Currently, most studies examining PN in the treatment of large tumors reveal its oncologic safety is similar to RN. Gilbert et al. [20] reported the oncologic outcomes of 82 patients with pT3a tumors—with 14 patients being managed by PN—however, the distinct findings of PN were not separately considered. They showed that pT3a tumors (with perinephric fat invasion) had recurrence and survival rates equivalent to those of pT1a tumors, regardless of the surgical method. Robert et al. [21] reported on 186 patients with cT1 lesions who had undergone nephrectomy. The 125 patients with pT1 and 57 with pT3a lesions had similar 5-year recurrence and survival rates. However, the investigators performed no analysis of the surgical method. Jeldres et al. [22] reported the results of 72 pT3a tumors treated by the PN technique compared with 789 patients who were managed by the RN technique and concluded that PN does not lower CSS. Hansen et al. [23] conducted a study reported in 2012 that described 477 pT3a tumors treated with PN compared with 477 pT3a tumors treated with RN and found no statistically significant differences in cancer-specific mortality at 2 and 5 years of follow-up. The mean follow-up period in previous studies was under 60 months, but the mean follow-up period in our study was 129 months. We observed that the operative method used—PN and RN— was not a significant predictor of recurrence and survival. However, only the tumor size was a found to be a significant factor in predicting disease recurrence and cancer-specific death in patients with pT3a RCC by the multivariate Cox proportional hazard model after controlling other variable factors.
Our study has some limitations. First, it was retrospective in nature. Second, a surgical selection bias was also present in this study. We performed PN on significantly smaller tumors than those treated with RN (mean, 3.1 cm vs. 7.0 cm, respectively; p<0.001). The clinically large renal tumors were mainly in the RN cohort. However, in our multivariate analysis, tumor size was the only significant factor for predicting disease recurrence and cancer-specific death. Additionally, there are large-scale studies comparing the prognosis of pT3a RCC according to surgical method, but there are no large-scale studies that assess pT3a without renal vein thrombus. The particularly small number of cT3a RCC cases in the PN cohort should be validated in large-scale future studies.
CONCLUSIONS
Based on the present findings, PN has similar RFS and CSS compared with RN among patients with pT3a RCC without renal vein thrombus. Additionally, our study shows that tumor size is the only factor affecting RFS and CSS after surgery. If there is no thrombus in the renal vein, there is no reason not to perform PN for cT3a tumor.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print



