

INTRODUCTION
Prostate cancer is the most frequently diagnosed solid tumor worldwide and the second leading cause of cancer-related deaths among the male population [1]. Most patients are diagnosed with localized cancer. However, some patients develop metastatic disease after the treatment of localized cancer. Moreover, 8% of patients are diagnosed with de novo metastatic hormone-sensitive prostate cancer (mHSPC) [2].
Over the past 15 years, the treatment of metastatic prostate cancer has undergone drastic changes owing to the development of androgen receptor-targeted agents (ARTA) and immuno-targeting agents [3-5]. Based on the development of these drugs, large-scale randomized controlled trial studies using or combining chemotherapy and ARTA have been recently conducted in patients with mHSPC. Therefore, various treatments have progressed away from androgen deprivation therapy (ADT), which was traditionally used to treat mHSPC [6,7].
ARTAs were initially studied in patients with metastatic castration-resistant prostate cancer (mCRPC). In mCRPC, docetaxel chemotherapy has been the preferred firstline drug since the TAX327 study [8]. However, after the publication of the COU-AA-302 [9] and PREVAIL studies [10] conducted in patients with mCRPC who had not received chemotherapy, the introduction of ARTA as a firstline treatment was one of the major changes in mCRPC treatment. In chemo-naive patients with mCRPC, ARTA resulted in a statistically significant improvement in overall survival (OS) [9,10] In addition, the use of ARTA was relatively advantageous even in patients who had difficulty receiving chemotherapy for various reasons [11].
Although it is clear that ARTA helps increase OS in these patients, in practice, some patients still show early disease progression [12]. It is difficult to predict the duration of treatment response to these ARTAs. Therefore, it will be of great help to know the predictive factors when using ARTA as the first-line treatment for mCRPC. Therefore, we investigated the data of patients with mCRPC who received ARTA without chemotherapy at Inha University Hospital. We studied the factors predicting the drug effect-response period of ARTA in mCRPC.
MATERIALS AND METHODS
1. Patients and Study Design
We retrospectively retrieved clinical and pathological data of patients with prostate cancer who received ARTA for mCPRC at Inha University Hospital between January 2010 and January 2023. The Institutional Review Board (IRB) of the Inha University Hospital approved this study (IRB approval No. 2023-07-034). Patients who received chemotherapy before ARTA and those with incomplete pathological or follow-up data were excluded from the study.
mCRPC is defined as the presence of castration levels of testosterone (50 ng/dL or 1.7 nmol/dL) and an increase in prostate-specific antigen (PSA) by more than 50% with 2 consecutive measurements at least 1 week apart and an absolute value of 2.0 ng/dL. Radiographic progression was defined as 2 or more new bone lesions on bone scans or new soft-tissue lesions using the Response Evaluation Criteria for Solid Tumors (RECIST). The clinical characteristics of these patients, including age, body mass index, initial PSA at diagnosis, PSA kinetic, International Society of Urological Pathology grade group (ISUP GG), visceral metastasis, bone metastasis, and lymph node (LN) metastasis (regional and nonregional) were obtained through a review of medical records. In most patients, the initial PSA changes after using ARTA were greatest. Thus, the PSA kinetic was determined based on the change value 3 months after using ARTA.
2. Follow-up
Follow-up was calculated from the time of the start of ARTA to the date of the last known contact with the patient or the date of death. During the follow-up period, PSA level measurement, sequential radiography such as computed tomography (CT) or magnetic resonance imaging (MRI), and bone scanning were performed for efficacy evaluation every 3 months. The currently used ARTA was discontinued, and the regimen was changed to another drug such as another ARTA or chemotherapy, when 2 or more of the following were observed: PSA elevations, radiologic progression, and worsening of clinical symptoms. Radiographic progression was defined as progression in softtissue lesions as measured using CT or MRI, according to RECIST criteria, or progression on bone scanning according to criteria adapted from the Prostate Cancer Working Group 3.
3. Statistical Analysis
We compared clinical and pathological characteristics between groups by using Mann-Whitney U-tests for continuous data and χ2 tests for dichotomous variables. Univariate and multivariate logistic regression analyses were performed to assess the association between baseline parameters and residual cancer. Significant variables in the univariate analysis were included in the multivariate analysis. In addition, the Kaplan-Meier method and log-rank test were performed in parallel to estimate and compare the OS rate according to the ARTA response. A p-value of <0.05 was considered statistically significant. Statistical analyses were performed using IBM SPSS Statistics ver. 23.0 (IBM Co., Armonk, NY, USA).
RESULTS
1. Patient and Disease Characteristics
Seventy patients with mCRPC received ARTA without chemotherapy and were included in the study. The median follow-up duration from ARTA start was 16.95±13.79 months. The mean age for all patients was 76.07±8.09 years. Among the pathology specimens, 5 (7.1%) exhibited ISUP GG 3, 18 (25.7%) exhibited ISUP GG 4, and 47 (67.1%) exhibited ISUP GG 5.
The mean initial PSA value at the diagnosis of prostate cancer was 355.64±788.54 ng/mL. At the time of ARTA initiation, 62 patients (88.6%) had bone metastases, 30 (42.9%) had visceral metastases, and 39 (55.7%) had LN metastasis. Among them, 17 had limited regional LN metastasis and 22 had nonregional LN metastasis. The mean ARTA treatment period until discontinuation owing to cancer progression was 334.9±364.71 days.
We divided the patients into 2 groups, early and late progression groups, according to the cancer response period to ARTA for 12 months. There were 44 and 26 patients in the early and late progression groups, respectively. The characteristics of each group are summarized in Table 1.
2. OS Following First ARTA Response Duration for Prechemo mCRPC
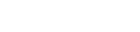
During the follow-up period, cancer-specific deaths were observed in 18 patients (25.7%); 11 and 7 patients in the early and late progression groups, respectively, had cancer-specific deaths. Additionally, the Kaplan-Meier curves showed a significant increase in OS in the late progression group for ARTA (log-rank test, p=0.001) (Fig. 1).
3. Predictors Associated With First ARTA Response Duration for Prechemo mCRPC
In this study, we used univariate and multivariate logistic regression analyses to identify predictors of ARTA response duration.
In these analyses, age (odds ratio [OR], 1.154; 95% confidence interval [CI], 1.043-1.251; p=0.005) and nonregional LN metastases (OR, 8.819; 95% CI, 1.165-66.746; p=0.035) were independent predictors of ARTA response duration in prechemo mCRPC in both univariate and multivariate models (Table 2).
DISCUSSION
Currently, the primary standard treatments for mCRPC are chemotherapy and ARTA [13]. Although no direct randomized controlled trials (RCT) study has been conducted among these treatments, it is difficult to determine which treatment is superior through a meta-analysis [14,15]. Therefore, the optimal treatment of mCRPC has not been determined. Both ARTA and chemotherapy have become standard treatments, and currently, the choice of drugs depends on the clinician’s judgment.
The usefulness of ARTA for oncologic outcomes in chemotherapy-naive patients with mCRPC has already been demonstrated in large-scale RCTs [9,10]. However, some studies have shown that docetaxel-based chemotherapy has a good prognosis in patients with mCRPC. In particular, studies have reported that patients with a high tumor burden respond poorly to ARTA [16,17]. However, the definition of high tumor burden is ambiguous across studies. Additionally, not all patients can withstand the adverse effects of chemotherapy [18]. Therefore, ARTA may be the preferred treatment for these patients. The choice of the first-line agent in patients with mCRPC is important when considering their response to subsequent treatment. The response to subsequent treatment is unlikely to be better than that of the first treatment. Cross-resistance between treatments, reported in previous studies, is thought to be one of the causes [19]. Antonarakis et al. [20] suggested that the levels of androgen receptor splice variant 7 (AR- V7) in circulating tumor cells are a potentially informative pretreatment prognostic marker [20]. Although the exact mechanisms have not yet been revealed [21], our study showed similar results. For this reason, research on the optimal sequence continues and clinical trials such as the OSTRICh study (NCT03295565), are underway to find the optimal subsequent treatment for patients with mCRPC with poor prognosis [22]. Therefore, it is of great significance to study the factors that predict the response duration to ARTA as the first treatment and determine appropriate treatment sequences for each patient.
In our study, older patients with mCRPC and those with nonregional LN metastases appeared to have poor therapeutic responses to ARTA without chemotherapy. In addition, in our study, OS was low in patients with early progression with first-line ARTA. Previous studies have also predicted responses to ARTA. Verzoni et al. [23] analyzed data from an Italian multicenter database. They reported that the duration of abiraterone response in mCRPC significantly correlated with PSA and ISUP GG. Kato et al. [24] reported that patients with early PSA response to enzalutamide had a good prognosis. Additionally, one study reported that the duration of ADT uses until progression to CRPC had an effect [25]. However, these studies were not limited to prechemotherapy patients with CRPC. A recent study published by Jeong et al. [26] reported that the use of abiraterone in patients with mCRPC before chemotherapy resulted in better results after chemotherapy. Considering the aforementioned cross-resistance, there may be differences between patients with mCRPC without chemotherapy and with chemotherapy. There are few studies on the factors predicting ARTA response duration in chemo-naive patients with mCRPC such as the present study.
Based on our results, we believe that the presence or absence of nonregional LN metastasis has a significant impact on the treatment response to ARTA in chemo-naive patients with mCRPC. Similar to our findings, a previous study published by Ali et al. [27] found that prostate cancer patients with M1a and M1b stages had poor prognoses. Because their study was conducted on patients with mHSPC, it differs from ours. However, because most patients in our study also had M1b, the poor prognosis of patients with M1a and M1b was similar in both studies. Therefore, we believe that it is similar to the aim of our study that patients with M1a and M1b tumors should be considered for more aggressive combination therapy.
Age also showed a statistically significant difference in our study. However, most of the patients included in our study were elderly, with an average age of 76.07±8.09 years. Therefore, it was difficult to perform the analysis based on the age of 75 or 70 years, as in previous studies [28]. In this study, age statistics were conducted using continuous variables, and since all patients were elderly, we think it is difficult to attach great significance to this result. Relatively young patients were indeed treated with ARTA for a long period; however, as in previous studies, the elderly patients included in this study also had no major side effects while using ARTA. Therefore, the use of ARTA is considered safe for elderly patients.
Our study had several limitations. First, this was a retrospective review of data from patients with prostate cancer treated at a single institution, and the number of patients included was small. Therefore, our results were affected by a selection bias, which limits their generalizability, and a multicenter prospective study is warranted. For these reasons, our findings may differ from previous RCT studies [9,10]. For example, it was not statistically significant in patients with visceral metastases. However, our study also showed a tendency for early progression in patients with visceral metastasis. Therefore, we do not mean that it is different from previous RCT studies. In addition, the enrolled patients in the current study were mostly diagnosed with mCRPC that occurred after using only ADT for mHSPC, and the study was limited to mCRPC without chemotherapy. Therefore, it may be difficult to apply the results of this study to patients with mHSPCs. Lastly, in our study, we were unable to conduct a comparative analysis of treatments other than ARTA in mCRPC patients with nonregional LN metastasis. Therefore, in order to find a better treatment, it would be meaningful to conduct additional comparative analysis on ARTA monotherapy and chemotherapy or ARTA and chemotherapy combination therapy.
Numerous studies have been conducted on mHSPC. Based on these studies, ARTA, chemotherapy, or combination therapy is used in patients with mHSPC [29,30]. Therefore, the number of chemo-naive patients with mCRPC may gradually decrease. However, there are still patients using ADT alone for mHSPC and patients developing mCRPC while using ADT after treatment for localized prostate cancer. Therefore, the first-choice treatment for patients with mCPRC is still important. We believe that this study provides valuable information for patients and clinicians.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print



