

INTRODUCTION
Renal cell carcinoma (RCC) is the most common neoplasm in the kidney, accounting for almost 4% of all incident malignancies in adults [1]. In the United States, an estimated 79,000 patients were newly diagnosed with RCC in 2022, among whom 13,920 died [1]. RCC often extends into the renal vein, forming a thrombus that can further progress into the inferior vena cava (IVC). A venous thrombus in the IVC was observed in approximately 10% of patients with RCC at the time of diagnosis [2].
Radical nephrectomy with thrombectomy (RNTx) is considered an effective treatment option for RCC with venous thrombus [3]. However, it is accompanied by surgical challenges, including the risk of massive bleeding, and the potential need for cardiopulmonary bypass in cases of highlevel tumor thrombus [4]. Although the 5-year survival rates after surgical management exceeded 50%, the postoperative mortality rates also reached almost 50% [5].
Several studies have been conducted to identify perioperative and postoperative prognostic factors for RCC with venous thrombus or RNTx, including operation time, vascular resection margin, sarcomatoid differentiation, tumor necrosis, venous thrombus level, TNM stage, and the histologic type of RCC [6-8]; however, the findings remain highly debated.
In this study, we retrospectively reviewed the medical records of RCC patients with venous thrombus who underwent RNTx at a single tertiary referral medical center over 30 years. We aimed to identify prognostic factors for cancer-specific survival (CSS).
MATERIALS AND METHODS
1. Study Population
This retrospective study reviewed the medical records of patients diagnosed with RCC with venous thrombus who underwent RNTx at a single tertiary medical center between January 1990 and December 2022. This study was approved by the Institutional Review Board of Asan Medical Center, and the requirement for informed consent from patients was waived due to the retrospective nature of the study (2023-1310).
The parameters included age, sex, lateralization of tumor location, tumor size, level of venous thrombus, histologic subtype, TNM stage, Fuhrman nuclear grade, presence of sarcomatoid differentiation, presence of lymphovascular invasion, presence of tumor necrosis, presence of a positive renal vein resection margin, date of final follow-up, and CSS and overall survival (OS). Preoperative computed tomography (CT) or magnetic resonance imaging reports from radiologists were reviewed to determine the size of the tumor, as well as the presence and level of venous thrombus. These reports were manually reviewed again for accuracy. The pathologic report was examined to determine the histologic type, Fuhrman nuclear grade, presence of sarcomatoid differentiation, presence of lymphovascular invasion, presence of tumor necrosis, and presence of positive renal vein resection margin. The TNM stage was determined according to the 2017 American Joint Committee on Cancer (AJCC) TNM classification system [9]. The histologic subtype was categorized as clear cell RCC, papillary RCC, chromophobe RCC, and other types of RCC. The Fuhrman nuclear grade was categorized as grades 1 and 2, grade 3, and grade 4. The surgical method for RNTx included open RNTx, laparoscopic RNTx, and hand-assisted laparoscopic RNTx. Robot-assisted RNTx was not performed.
The venous thrombus level data were also collected and classified according to the Mayo classification system [10], as follows: level 0, venous thrombus is limited to the renal vein; level 1, venous thrombus extends into the IVC to no more than 2 cm above the renal vein; level 2, the venous thrombus extends into the IVC to more than 2 cm above the renal vein but below the hepatic vein; level 3, venous thrombus extends into the IVC to above the hepatic vein but below the diaphragm; level 4, the venous thrombus extends above the diaphragm or right atrium. CT images before RNTx were used to calculate the venous thrombus level.
2. Statistical Analyses
Continuous data are presented as the median with the interquartile range (IQR), and categorical data are presented as the number and percentage of patients. Univariate and multivariate Cox proportional hazard regression analyses were used to identify significant prognostic factors affecting CSS. The hazard ratio (HR) and 95% confidence interval (CI) were used for the results of the univariate and multivariate Cox proportional hazard regression. A Kaplan-Meier model was used to calculate CSS rates at 1, 3, and 5 years after RNTx. Statistical significance was set at p<0.05. All statistical analyses were performed using IBM SPSS Statistics ver. 23.0 (IBM Co., Armonk, NY, USA).
RESULTS
1. Baseline Characteristics of the Study Population
A total of 262 patients who had RCC with venous thrombus were identified (Table 1). The median patient age was 59 years (IQR, 51-67 years) and comprised 80.15% (210 of 262) male and 19.85% (52 of 262) female patients. There were 110 right-sided tumors (41.98%) and 152 leftsided tumors (58.02%). The median tumor size was 9.5 cm (IQR, 7.5-11.6 cm). The histopathologic findings were reported as follows: clear cell RCC in 211 patients (80.53%), papillary RCC in 17 patients (6.49%), chromophobe RCC in 6 patients (2.29%), and other types of RCC in 28 patients (10.69%). Among them, 36 patients (13.74%) were staged as T4, 56 (21.37%) as N1, and 68 (25.95%) as M1. The venous thrombus was level 0 in 97 patients (37.02%), level 1 in 64 (24.43%), level 2 in 42 (16.03%), level 3 in 30 (11.45%), and level 4 in 29 (11.07%). The Fuhrman nuclear grade was grade 1 or 2 in 35 patients (13.36%), grade 3 in 108 (41.22%), and grade 4 in 115 (43.89%). Sarcomatoid differentiation was present in 58 patients (22.14%), lymphovascular invasion in 176 (67.18%), and tumor necrosis in 152 (58.02%). Furthermore, the renal vein resection margin was pathologically positive in 72 patients (27.48%). The operation period was categorized based on the year in which patients underwent RNTx (through the end of 2011, in 2012 and beyond). The number of patients who underwent RNTx through the end of 2011 was 129, while 133 patients underwent RNTx in 2012 and beyond.
2. Cancer-Specific Survival
Cox proportional hazard model data for CSS are presented in Table 2. In the univariate analysis, papillary histologic type (HR, 2.306; 95% CI, 1.225-4.341, p=0.01), pathologic T4 stage (HR, 2.171; 95% CI, 1.345-3.504; p=0.002), pathologic N1 stage (HR, 1.928; 95% CI, 1.270-2.929; p=0.002), pathologic M1 stage (HR, 2.643; 95% CI, 1.811-3.857; p<0.001), Fuhrman nuclear grade 4 (HR, 1.607; 95% CI, 1.113-2.321; p=0.011), sarcomatoid differentiation (HR, 2.111; 95% CI, 1.211-3.680; p=0.008), lymphovascular invasion (HR, 2.084; 95% CI, 1.117-3.889; p=0.021), tumor necrosis (HR, 3.813; 95% CI, 1.667-8.721; p=0.002) and pathologic renal vein resection margin positivity (HR, 1.560; 95% CI, 1.063-2.288; p=0.023) were significantly associated with CSS. In the multivariate analysis, pathologic T4 stage (HR, 3.711; 95% CI, 1.599-8.611; p=0.002), pathologic N1 stage (HR, 2.371; 95% CI, 1.231-4.567; p=0.01), sarcomatoid differentiation (HR, 1.890; 95% CI, 1.027-3.477; p=0.041) and tumor necrosis (HR, 2.993; 95% CI, 1.132-7.914; p=0.027) were statistically associated with CSS.
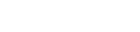
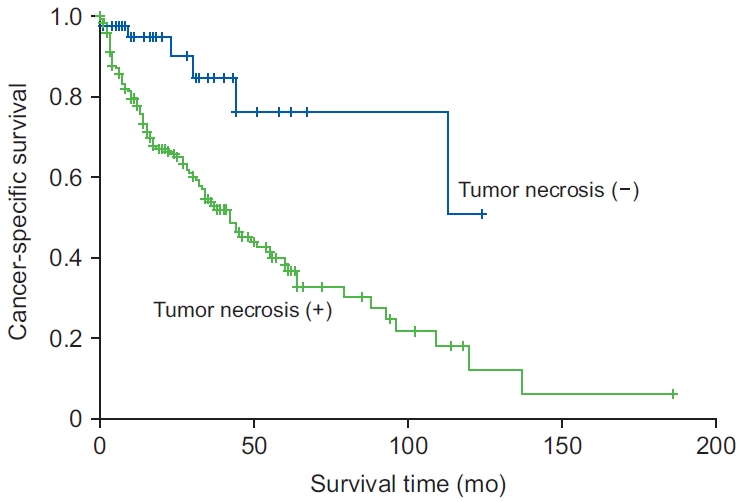
The Kaplan-Meier results for CSS according to pathologic T4 stage, pathologic N1 stage, sarcomatoid differentiation, and tumor necrosis, which were significantly associated with CSS in the multivariate analysis, are presented (Figs. 1-4), respectively. For pathologic T4 stage, the 1, 3, and 5-year CSS rates were 60.8%, 39.4%, and 21.9%, respectively, compared with 85.9%, 63.9%, and 48.1%, respectively for patients with pathologic T stage under 4 (p=0.001). For pathologic N1 stage, the 1, 3, and 5-year CSS rates were 83.8%, 37.1%, and 27.9%, respectively, compared with 85.8%, 67.1%, and 49.2%, respectively, for patients with pathologic N0 disease (p=0.002). For sarcomatoid differentiation, the 1, 3, and 5-year CSS rates were 71.0%, 47.3%, and 36.8%, respectively, compared with 89.6%, 69.6%, and 52.0%, respectively, in patients with no sarcomatoid differentiation (p=0.007). For tumor necrosis, the 1, 3, and 5-year CSS rates were 79.6%, 53.8%, and 38.3%, respectively, compared with 94.8%, 84.8%, and 76.3%, respectively, in patients with no tumor necrosis (p=0.001).
DISCUSSION
The analysis of pathological reports in this study revealed that pathologic T4 stage, pathologic N1 stage, sarcomatoid differentiation, and tumor necrosis were associated with poor CSS. Furthermore, tumor size, histologic type of RCC, Fuhrman nuclear grade, thrombus level, lymphovascular invasion, and positive renal vein resection margin were not associated with CSS.
Our findings showed that the venous thrombus level was not associated with CSS, which has been reported in several studies [11,12]. Shiff et al. [11] reported that venous thrombus level was not a significant prognostic factor for CSS, even for recurrence-free survival (RFS) and OS in 228 nonmetastatic RCC patients with venous thrombus who underwent RNTx. They categorized patients into 3 groups according to venous thrombus level (level 0, levels 1-2, and levels 3-4), and found no significant differences in CSS, RFS, or OS among the 3 groups. Klatte et al. [12] also concluded that venous thrombus level was not a prognostic factor for CSS. After identifying the medical records of 321 RCC patients with venous thrombus who underwent RNTx at a single medical institution, the patients were categorized into 3 groups based on thrombus level, classified as renal vein thrombus, IVC thrombus, and right atrium thrombus. We observed no association between venous thrombus level and CSS. In contrast, Mager et al. [13] reported that venous thrombus level was significantly associated with CSS, similar to pathologic N stage, distant metastasis, and perinephric fat invasion. They retrospectively reviewed the medical reports of patients who had RCC with venous thrombus and underwent RNTx at 16 institutions across the United States and Europe. In their study, they excluded patients who had RCC with venous thrombus limited to renal vein thrombus. This exclusion might have increased the average venous thrombus level, leading to opposite outcomes compared with our study. Tang et al. [14] also reported that the venous thrombus level was a prognostic factor for CSS in the entire population and nonmetastatic subgroup. Furthermore, the level 2 subgroup had a better prognosis than the level 3 and 4 subgroups, and the level 1 and 2 subgroups had a better prognosis compared with the level 3 and 4 subgroups. In their study, patients categorized as stage T4 and those who underwent palliative cytoreductive nephrectomy were excluded. This might have led to a relatively small number of patients with lower severity, who had higher venous thrombus levels, possibly explaining their results, which were inconsistent with our own.
Yang et al. [15]. reported on the significance of sarcomatoid differentiation in RCC patients with venous thrombus who underwent RNTx. In this retrospective study at a single institution involving 125 patients, RCC with sarcomatoid differentiation tended to lead to worse progression-free survival (PFS) and CSS than RCC without sarcomatoid differentiation. Sarcomatoid differentiation was associated with larger tumor size, a higher risk of necrosis, and a higher tumor stage, and was also more frequently observed in clear cell RCC [16]. The proportion of patients with metastasis in our study was 26%, and we identified sarcomatoid differentiation as a significant factor. The relationship between sarcomatoid differentiation and RCC metastasis remains a matter of debate. Sarcomatoid differentiation was also associated with PFS and OS in metastatic RCC, and it predicted a poor response to target therapy in metastatic RCC [16,17]. Thus, we hypothesized that there is an association between metastasis of RCC and sarcomatoid differentiation.
Zhang et al. [18] conducted a meta-analysis that identified a significant association between histologic tumor necrosis and CSS, OS, RFS, and PFS in patients with RCC. They reviewed 34 studies investigating the relationship between RCC and tumor necrosis and concluded that tumor necrosis could be a poor prognostic factor for RCC. The proportion of tumor necrosis was related to the degree of intratumoral hypoxia, resulting from the rapid growth of the tumor outpacing the growth of the blood vessels. Tumor necrosis was associated with a poor prognosis and a higher likelihood of vulnerability to radiotherapy and chemotherapy [19]. In our study, the 5-year survival rate for patients with no tumor necrosis was 76.3%, which exceeded the average 5-year survival following RNTx. Coons et al. [20] reported that tumor necrosis in the pathologic report was associated with OS, CSS, and RFS. They highlighted that patients who had no tumor necrosis had better OS, CSS, and RFS outcomes, particularly with a 5-year survival rate exceeding 60% compared with the overall CSS and RFS rates, which were approximately 50%. Their study included over 100 patients with T3b RCC according to the 2002 AJCC TNM staging criteria, wherein the tumor involves the renal vein or vena cava below the diaphragm, corresponding with the T3a and T3b 2010 TNM staging criteria [21]. Additionally, their patients had similar stage and metastasis ratios. Nevertheless, the 5-year CSS in patients with tumor necrosis was approximately 25% in their study, compared with 38.3% in ours. The higher survival rates for tumor necrosis and the absence of tumor necrosis in our study can be attributed to their use of patient data from 1988 to 2006, whereas our study covered the period from 1990 to 2022. Across these different periods, there might have been variations in surgical skills, surgical instruments, and postoperative care, leading to more favorable survival outcomes.
In our previous report in 2010 [22], we discussed the surgical and survival outcomes following RNTx. We concluded that tumor thrombus level was not significantly associated with OS, a finding consistent with our current study. However, pathologic T stage was also not a significant prognostic factor for OS in our previous study, but it did emerge as significant in our current study. This could be attributed to an increase in the number of patients analyzed in this study compared with the previous analysis.
Our study had several limitations. First, it was a retrospective review conducted at a single institution, which risks selection bias; however, we evaluated a larger number of patients than in other single-institutional studies on RNTx. Next, our study included a heterogeneous group of patients, and we could not conduct a subgroup analysis owing to the insufficient number of cases. Additionally, we did not have information on medical treatment. However, despite the limitations of our single-institutional study, there was low variability in surgical factors, enabling a detailed review with long-term follow-up.
CONCLUSION
In this retrospective study conducted at a single tertiary referral center, focusing on RCC patients with venous thrombus who underwent RNTx, pathologic T4 stage, pathologic N1 stage, sarcomatoid differentiation, and tumor necrosis were identified as significant prognostic factors for CSS. However, the venous thrombus level was not significantly associated with CSS. Further prospective studies are warranted to elucidate the prognostic factors for CSS in RCC patients with venous thrombus who undergo RNTx.



 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print



