

INTRODUCTION
According to a report from the early 2000s, 10,246 cases of primary bladder cancer occurred in Korea from 1998 to 2002. Furthermore, based on the 2021 Korea National Cancer Incidence Database, bladder cancer is the cancer with the 10th highest burden of incidence and mortality in men [1].
Twenty-five percent of patients who are newly diagnosed with bladder cancer have muscle-invasive bladder cancer. The leading treatment for muscle-invasive bladder cancer or refractory high-grade non-muscle-invasive bladder cancer patients is generally radical cystectomy (RC) with extended bilateral lymphadenectomy. With pathological staging, this procedure can provide an exact evaluation of both bladder cancer and the regional lymph nodes (LNs). Several variables have been identified as significantly related to the disease-specific survival of bladder cancer. LN metastasis, in particular, has been considered as a predictor of bladder cancer-related survival [2,3]. Several studies have established variables that can be used to predict an adverse prognosis, such as age, tumor stage and LN density, which are used to calculate the COBRA (Cancer of the Bladder Risk Assessment) score [4]. Along with the prognostic value of factors related to the LNs, lymphovascular invasion and angiolymphatic invasion (ALI) remain a matter of debate. ALI has been identified as a poor prognostic factor for other solid tumors, such as upper urinary tract, prostate, liver, and colorectal cancer [5,6]. Based on the concept that angiolymphatic channels allow the dissemination of invading tumor cells, several articles have reported poor prosnosis for cases of bladder cancer in which RC or even transurethral resection was performed [7]. However, other studies have found ALI not to be significant in comparison to other variables [8] or less significant for urothelial bladder cancer than for squamous cell carcinoma of the bladder [9].
In this study, we aimed to evaluate the prognostic value of ALI in cases of bladder cancer treated with RC.
MATERIALS AND METHODS
1. Study Population
The retrospective, multicenter, full-scale survey study analyzed 495 patients who underwent robot-assisted radical bladder cystectomy between April 2007 and October 2019. The study was approved by the Institutional Review Board of Bundang Seoul National University Hospital (IRB no. 2019AN0102). Of the 495 patients, ALI was present in 182 patients and absent in 313 patients. The exclusion criteria were non-transitional cell carcinoma histology, a history of neoadjuvant therapy, and incomplete data. The surgical technique and the extent of lymphadenectomy (standard, extended, or limited) were decided based on the surgeon's discretion. Regional lymphadenectomy was also performed based on preoperative imaging or an intraoperative examination.
2. Data Collection and Pathologic Evaluation
Clinical and pathological information was also retrospectively obtained from individual medical records from corresponding hospitals for bladder cancer research (a total of 7 medical institutions). Staff pathologists from each institution examined all specimens according to the institutional protocol. The American Joint Committee on Cancer/TNM classification system was used for pathological staging, and the World Health Organization classification was used for pathological staging. The clinicopathologic data included age, sex, comorbidity, tumor stage, tumor grade, surgical margin, presence of ALI, perineural invasion, squamous or glandular metaplasia, and the presence of carcinoma in situ (CIS). ALI was defined as the presence of tumor cells within an arterial, venous, or lymphatic lumen. ALI presence was assessed using routine light microscopic examinations with hematoxylin and eosin staining.
3. Statistical Analyses
Descriptive statistics were calculated to evaluate any potential differences in the demographic data and health status of the subjects.
We divided the patients into ALI and non-ALI groups based on the primary tumor. Differences between these 2 groups were evaluated by the chi-square test for categorical variables and the independent t-test for continuous variables. The Kaplan-Meier method was used to calculate time-dependent outcomes, such as recurrence-free survival (RFS), cancer-specific survival (CSS), and overall survival (OS) and differences were assessed with the log-rank statistic. Univariate and multivariate survival analyses were performed with a Cox proportional-hazards regression model to evaluate the prognostic significance of the pathological variables. Statistical significance in this study was set at p<0.05. All analyses were performed with IBM SPSS Statistics ver. 22.0 (IBM Co., Armonk, NY, USA).
RESULTS
1. Baseline Characteristics of Patients
The baseline characteristics of all 495 patients in this study are shown in Table 1. Their median age was 65 years, and the median and mean follow-up durations were 23.3 months and 37.1 months, respectively (range, 0-134 months). Most patients were men (418 patients, 84%). ALI was present in 182 patients (36.8%). The baseline characteristics of the ALI-negative group were similar to those of the ALI-positive group (n=313, 63.2%)
Table 1.
Baseline characteristics and perioperative outcomes among 496 patients who underwent radical cystectomy according to angiolymphatic invasion
| Characteristic | All (n=495) | Angiolymphatic invasion | p-value | |
|---|---|---|---|---|
| Yes (n=182) | No (n=313) | |||
| Age (yr) | 65.5±10.4 | 67.3±10.8 | 64.6±10.1 | 0.006* |
| BMI (kg/m2) | 24.1±3.1 | 23.8±3.4 | 24.3±2.9 | 0.205 |
| Sex | 0.558 | |||
| Male | 418 (84.4) | 148 (81.3) | 271 (86.6) | |
| Female | 77 (15.6) | 34 (18.7) | 42 (13.4) | |
| Smoking | 0.913 | |||
| Never | 259 (52.3) | 91 (50.0) | 168 (53.7) | |
| Former | 176 (35.6) | 65 (35.7) | 111 (35.5) | |
| Current | 60 (12.1) | 26 (14.3) | 34 (10.9) | |
| ASA PS classification | 0.006* | |||
| I | 154 (31.1) | 41 (22.5) | 113 (36.1) | |
| II | 306 (61.8) | 120 (65.9) | 186 (59.4) | |
| III | 35 (7.1) | 21 (11.5) | 14 (4.5) | |
| Preoperative GFR | 75.54 | 72.77 | 77.11 | 0.046* |
| Hydronephrosis | 0.001* | |||
| No | 373 (75.4) | 119 (65.4) | 252 (80.5) | |
| Yes | 122 (24.6) | 63 (34.6) | 61 (19.5) | |
| DM | 113 (22.8) | 47 (25.8) | 66 (21.1) | 0.160 |
| HTN | 211 (42.6) | 84 (46.2) | 127 (40.6) | 0.130 |
| Perioperative outcomes | ||||
| Operation time (min) | 434 | 424 | 440 | 0.236 |
| Estimated blood loss (mL) | 524 | 527 | 522 | 0.913 |
| Transfusion rate | 83 (16.8) | 33 (18.1) | 50 (16.0) | 0.444 |
| Complications | 298 (60.2) | 105 (57.7) | 193 (61.7) | 0.657 |
| ≥Grade 3 | 104 (21.0) | 32 (17.6) | 72 (23.0) | 0.210 |
The patients with ALI were significantly older (67.3 years vs. 64.6 years, p=0.006), had lower American Society of Anesthesiologists (ASA) physical status classification grades (ASA I: 22.5% vs. 36.1%, p=0.006) and had a higher rate of hydronephrosis (34.6% vs. 19.5%, p=0.001) than the patients without ALI. There were no significant differences in other characteristics, such as body mass index, sex, smoking history, preoperative glomerular filtration rate, or preexisting comorbidities (diabetes mellitus or hypertension) (Table 1).
2. Perioperative and Pathological Outcomes
Among a total of 495 patients who underwent robotic RC, there was no significant difference in average operation time (424 minutes vs. 440 minutes, p=0.236). In estimated blood loss, no significant difference was found (527 vs. 522, p=0.913). The patients with ALI had a higher rate of transfusion (18.1% vs. 16.0%, p=0.444) and a lower complication rate (57.7% vs. 61.7%, p=0.657), but without statistical significance (Table 1).
In terms of the final pathologic outcomes, the presence of ALI was associated with a significantly higher T stage (T3 or T4) and a significantly lower T stage (Ta to T2) (p<0.001). Similar relationships were observed for higher tumor grade, such as grade III (74.6% vs. 50.6%, p<0.001) and higher rates of LN invasion (48.1% vs. 10.4%, p<0.001) in the patients with ALI. The ALI-positive group also showed significantly higher frequencies of perineural invasion (37.6% vs. 8.9%, p<0.001), squamous metaplasia (11.6% vs. 6.6%, p=0.010), and glandular metaplasia (7.7% vs. 2.3%, p=0.001). In contrast, CIS was significantly more common in the ALI-negative group (0.6% vs. 17.0%, p<0.001). No significant difference was found in the percentage of positive surgical margins between the 2 groups (4.4% vs. 2.7%, p=0.185).
3. CSS, OS, and RFS Outcomes
Disease recurrence was observed in 153 patients (30.9%), and 70 patients (14.1%) were dead at the time of final follow-up (except for those lost to follow-up). Recurrence was significantly more common in patients with ALI than in those without ALI (38.5% vs. 26.5%, p<0.001)
The most frequent site of recurrence was the LN, with 47 patients (29.9%), followed by lung (23.6%), bone (17.2%) and liver and neobladder/conduit (12.7%). Other sites of recurrence included the ureter (4.5%) and urethra (3.2%). There was a single incidence of kidney, ureter, and urethra recurrence in the ALI-positive group. LN recurrence was also the most frequent site of recurrence in the ALI-negative group, with 29 patients (34.1%), but in the ALI-positive group, the lung was the most frequent site of recurrence (20 patients, 27.8%). However, no statistically significant differences were observed in recurrence sites between the 2 groups, except for the liver (p=0.017) (Table 2).
Table 2.
Pathological and oncological outcomes according to presence of angiolymphatic invasion among patients who underwent radical cystectomy
| Variable | All (n=440) | Angiolymphatic invasion | p-value | |
|---|---|---|---|---|
| Yes (n=181) | No (n=259) | |||
| Pathological outcomes | ||||
| T stage | <0.001* | |||
| Ta | 10 (2.3) | 0 (0) | 10 (3.9) | |
| T1 | 102 (23.2) | 8 (4.4) | 94 (36.3) | |
| T2 | 128 (29.1) | 40 (22.1) | 88 (34.0) | |
| T3 | 156 (35.5) | 101 (55.8) | 55 (21.2) | |
| T4 | 44 (10.0) | 32 (17.7) | 12 (4.6) | |
| Carcinoma in situ | 45 (10.2) | 1 (0.6) | 44 (17.0) | <0.001* |
| Lymph node invasion | 114 (25.9) | 87 (48.1) | 27 (10.4) | <0.001* |
| Grade | <0.001* | |||
| I | 51 (11.6) | 4 (2.2) | 47 (18.1) | |
| II | 70 (15.9) | 16 (8.8) | 54 (20.8) | |
| III | 266 (60.5) | 135 (74.6) | 131 (50.6) | |
| Positive surgical margin | 15 (3.4) | 8 (4.4) | 7 (2.7) | 0.185 |
| Perineural invasion | 91 (20.7) | 68 (37.6) | 23 (8.9) | <0.001* |
| Squamous metaplasia | 38 (8.6) | 21 (11.6) | 17 (6.6) | 0.010* |
| Oncological outcomes | All (n=495) | Yes (n=182) | No (n=313) | |
| Recurrence | 153 (30.9) | 70 (38.5) | 83 (26.5) | <0.001* |
| Recurrence site | ||||
| Neobladder/conduit | 20 (12.7) | 6 (8.3) | 14 (16.5) | 0.158 |
| Lymph node | 47 (29.9) | 18 (25.0) | 29 (34.1) | 0.293 |
| Lung | 37 (23.6) | 20 (27.8) | 17 (20.0) | 0.181 |
| Bone | 27 (17.2) | 14 (19.4) | 13 (15.3) | 0.427 |
| Liver | 20 (12.7) | 4 (5.6) | 16 (18.8) | 0.017* |
| Other | 63 (40.1) | 30 (41.7) | 33 (38.8) | 0.524 |
| Cancer-specific mortality | 39 (7.9) | 19 (10.4) | 20 (6.4) | 0.012* |
| Overall mortality | 70 (14.1) | 31 (17.0) | 39 (12.5) | 0.010* |
Of the 70 dead patients (14.1%), cancer-specific death was recorded in 39 patients. ALI was significantly related to lower RFS, CSS, and OS (p<0.001, p=0.012, and p=0.01, respectively).
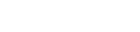
The ALI-negative patients showed higher 5-year and 10-year OS, CSS, and RFS. The exact percentages are given in Fig. 1. The mean OS was 95.7 months in the ALI-positive group versus 109.3 months in the ALI-negative group, the mean CSS was 108.7 months in the ALI-positive group versus 120.3 months in the ALI-negative group, and the mean RFS was 65.9 months in the ALI-positive group versus 89.1 months in the ALI-negative group (Fig. 1).
Fig. 1.
Oncological outcomes (OS, CSS, and RFS) according to presence of angiolymphatic invasion among patients who underwent radical cystectomy. OS, overall survival; ALI, angiolymphatic invasion; RFS, recurrence-free survival; CSS, cancer-specific survival.

Multivariate and univariate Cox proportional hazard models to predict bladder cancer recurrence and survival among all 495 patients in the study are shown in Table 3, with all variables calculated in the analysis. Tumor stage (over T2), ALI, and LN metastasis were all associated with bladder cancer-specific death in the univariate analysis. Adjusting for those significant variables, the multivariate analysis showed that tumor stage (over T2) and ALI were independent predictors of CSS (hazard ratio [HR], 1.632; 95% confidence interval [CI], 1.035-2.571, p=0.035; HR, 2.396; 95% CI, 1.256-4.571, p=0.008, respectively), while LN metastasis was not (p=0.209) (Table 3).
Table 3.
Uni- and multivariate Cox proportional hazard analysis among patients who underwent radical cystectomy for cancer-specific survival
| Variable | Univariate analysis | Multivariate analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-value | HR | 95% CI | p-value | |
| Age | 1.026 | 0.993-1.060 | 0.121 | - | - | - |
| Sex, female vs. male | 0.899 | 0.376-2.149 | 0.811 | - | - | - |
| Body mass index | 0.907 | 0.817-1.007 | 0.067 | - | - | - |
| Tumor stage, ≥T2 or not | 2.398 | 1.099-5.232 | 0.028* | 1.632 | 1.035-2.571 | 0.035* |
| Tumor grade, ≥2 or not | 1.652 | 0.638-4.276 | 0.301 | - | - | - |
| CIS+ | 0.962 | 0.340-2.720 | 0.942 | - | - | - |
| Angiolymphatic invasion | 2.253 | 1.191-4.260 | 0.012* | 2.396 | 1.256-4.571 | 0.008* |
| LN+ | 2.414 | 1.238-4.703 | 0.010* | 1.647 | 0.757-3.583 | 0.209 |
| Positive surgical margin | 1.530 | 0.208-11.241 | 0.676 | - | - | - |
| Preoperative GFR | 0.997 | 0.983-1.011 | 0.639 | - | - | - |
| Presence of preoperative DM | 1.529 | 0.760-3.076 | 0.234 | - | - | - |
| Presence of preoperative HTN | 0.723 | 0.371-1.408 | 0.340 | - | - | - |
| History of smoking | 1.702 | 0.899-3.223 | 0.103 | - | - | - |
For RFS, tumor stage (over T2), tumor grade (over grade 2), ALI, LN metastasis, and a positive surgical margin showed significant associations in the univariate analysis. The adjusted multivariate analysis showed that tumor stage over T2, ALI, LN metastasis, and positive surgical margin were independent predictors of RFS. Tumor grade (over grade 2) was not a significant predictor (Table 4).
Table 4.
Uni- and multivariate Cox proportional hazard analysis among patients who underwent radical cystectomy for recurrence-free survival
| Variable | Univariate analysis | Multivariate analysis | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-value | HR | 95% CI | p-value | |
| Age | 1.006 | 0.991-1.021 | 0.450 | - | - | - |
| Sex, female vs. male | 0.749 | 0.497-1.128 | 0.167 | - | - | - |
| Body mass index | 0.982 | 0.932-1.034 | 0.485 | - | - | - |
| Tumor stage, ≥T2 or not | 2.713 | 1.817-4.049 | <0.001* | 1.938 | 1.209-3.107 | 0.006* |
| Tumor grade, ≥2 or not | 1.700 | 1.030-2.805 | 0.038* | 1.087 | 0.580-2.037 | 0.794 |
| CIS+ | 0.780 | 0.442-1.378 | 0.393 | - | - | - |
| Angiolymphatic invasion | 1.875 | 1.361-2.582 | <0.001* | 1.717 | 1.071-2.753 | 0.025* |
| LN+ | 2.702 | 1.939-3.765 | <0.001* | 1.837 | 1.254-2.692 | 0.002* |
| Positive surgical margin | 2.910 | 1.425-5.943 | 0.003* | 4.090 | 1.831-9.137 | 0.001* |
| Preoperative GFR | 0.998 | 0.991-1.005 | 0.565 | - | - | - |
| Presence of preoperative DM | 1.003 | 0.682-1.475 | 0.988 | - | - | - |
| Presence of preoperative HTN | 0.805 | 0.579-1.118 | 0.195 | - | - | - |
| History of smoking | 1.074 | 0.782-1.474 | 0.660 | - | - | - |
DISCUSSION
Identifying prognostic factors associated with the survival and recurrence of bladder cancer is crucial for selecting among treatment options. Several guidelines include pathological stage, LN metastases, and tumor size as prognostic factors for survival and recurrence. However, the prognostic value of ALI for bladder cancer patients who have undergone RC remains a matter of debate. Some studies have shown that this pathological property was associated with worse survival outcomes [10-14], while others have reported discordant findings [8, 15-18]. A subgroup analysis showed that ALI was not correlated with lower RFS in Asian populations [19]. Canter et al. [20] demonstrated that ALI showed significance only in pT3 patients based on univariate analysis of OS, CSS, and RFS. In the multivariate analysis, ALI was also a significant predictor for worse OS and disease-specific survival (p<0.01 and p=0.007, respectively), but not for RFS (p=0.1). According to a multi-institutional retrospective study conducted by Lotan et al. [21], ALI showed significance for predicting survival and recurrence, specifically for LN-negative patients. They also reported that the prevalence of ALI was 9% in pT1 and 78% in pT4 disease. Our study also showed similar results for the prevalence of ALI (7.8% in pT1, 72.7% in pT4). Regarding the N stage, 72% of LN-positive patients had ALI, while only 26% of LN-negative patients had ALI. Similarly, our study showed that 76% of LN-positive patients were ALI-positive.
We retrospectively analyzed a multi-institutional database of patients who underwent RC to evaluate the influence of ALI on tumor survival and recurrence. ALI showed significant associations with poor OS, CSS, and RFS. The 5-year OS was 82.7% in patients without ALI and 75.7% in patients with ALI. The 10-year OS was 65.0% in patients without ALI and 58.9% in those with ALI. This aligns with other studies that reported lower 5-year or 10-year OS or CSS in patients with ALI [8,14]. Furthermore, in line with previous reports [19,21], ALI was pathologically found in 36% of specimens.
A multivariate analysis was also done to clarify whether ALI can serve as an independent prognostic factor for recurrence and survival. In our analysis, ALI was an independent predictor for both RFS and CSS in univariate analysis (p=0.025 and p=0.008, respectively). Other factors, such as tumor stage and LN metastasis, were also related to both RFS and CSS, and tumor grade and a positive surgical margin were also related to RFS in the univariate analysis. In the multivariate analysis, higher T stage, LN metastasis, ALI, and a positive surgical margin were significant factors associated with recurrence, while only higher T stage and ALI were significant factors associated with CSS. Bassi et al. [22] reported that tumor stage and LN metastasis (but not ALI) were valuable factors for predicting survival through a multivariate analysis. In contrast, Canter et al. [20] demonstrated that ALI-positive patients showed lower OS, CSS, and RFS in the univariate analysis (p<0.001), and only OS and CSS showed significance in the multivariate analysis (p<0.01 and p=0.007, respectively). As shown by the above summary, several studies have reported different findings for independent predictors of survival and recurrence depending on the analysis type.
In our study, ALI-positive patients had a tendency for recurrence in the LNs, followed by the lung, neobladder/conduit, bone, and liver. This pattern of recurrence or progression was previously shown by Elsayed et al. [23], where metastasis occurred most frequently in the LNs (5%) and lung (6%). However, given the limited number of studies on the relationship between ALI and the progression or recurrence site, further study would help analyze the relevance of ALI for local and distal recurrence patterns.
Several previous studies of patients with other urological cancers, such as penile and prostate cancer, have established a relationship between ALI in LN-positive patients and a poorer prognostic outcome [5]. As ALI is theoretically related to both the lymphatic and vascular systems, this pathological property can be strongly associated with cancer cell spread [24]. Based on this characteristic of ALI as an important prognostic factor, the TNM staging for some cancers includes ALI. This may facilitate more precise cancer staging and improved decision-making by physicians. There has also been some debate about including ALI in the TNM staging of bladder cancer, based on studies that showed ALI to have prognostic value for worse progression-free survival and OS in RC patients (pooled HRs of 1.57 and 1.59, respectively) [25,26]. However, due to the difficulty of assessing ALI at a morphological level and the rare clinical use of immunohistochemical markers that enable differentiating lymphatic and vascular invasion at the pathological level, ALI is not yet appropriate for inclusion into the TNM staging system [27,28].
This study has several limitations. First, as a retrospective study, there is a risk of inherent bias. As this was a multicenter study, the pathological reports from each center for ALI may have been different or the criteria of ALI may have changed during the 12-year follow-up period. It is important to propose absolute morphological criteria to define ALI as vascular invasion or lymphatic invasion or combined in a standardized manner.
Our study also did not assess the extent of pelvic LN dissection, which may have generated bias; however, previous reports have shown no difference in RFS, CSS, or OS between extended and limited PLND [29]. However, these results remain uncertain. Even though extended LND is considered a standard procedure for RC, differences in the extent of PLND might affect the outcomes. The bias incurred by this limitation may have influenced our results for the relationship between LN metastasis and CSS. Fewer than 10 nodes were dissected in 101 out of 440 cases, corresponding to the lowest nodal yield for determining surgical quality. This result demonstrates that an inappropriate PLND extent and deficiency of the nodal yield might have influenced the results, as a bias incurring a higher likelihood for false negatives. Additional information will be needed on how to define the range of PLND.
Finally, since therapeutic options have changed rapidly since the 2000s, our study's long follow-up may not have accurate implications for newly diagnosed patients. The follow-up period of this study marks a transition from the beginning to the middle of robotic surgery. The learning curve for surgery might have biased the outcomes. Regarding this limitation, future large-scale randomized prospective trials with stringent criteria will provide insights into the effects of ALI on patients’ prognoses.
CONCLUSIONS
In conclusion, the presence of ALI in bladder cancer patients who underwent RC was associated with significantly worse outcomes both in terms of survival and recurrence.
Furthermore, along with a high T stage, the presence of ALI was an independent predictor influencing both CSS and RFS. Future prospective studies should be performed to further validate our results.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print



